
Breaking the Hand-Foot-and-Mouth Narrative
How Medicine Rebranded Vaccine Injury as Infectious Disease


Section 1: The Unquestioned Narrative
Hand-foot-and-mouth disease presents a compelling case study in how medical orthodoxy creates and perpetuates narratives without rigorous scientific validation. We're told it's a highly contagious viral illness caused by enteroviruses, particularly coxsackievirus A16 and enterovirus 71, spreading rapidly through daycare centers and preschools. The CDC confidently states that the virus spreads through contact with respiratory droplets, blister fluid, and fecal matter. Parents are warned to keep their children home, doctors prescribe supportive care while waiting for the "virus" to run its course, and everyone accepts this explanation without question.
Yet when we examine the actual evidence for these claims, we find ourselves standing on remarkably shaky ground. The foundational studies claiming to identify the causative virus follow the same flawed methodology that virologists have used since 1954 - mixing patient samples with monkey kidney cells, fetal bovine serum, antibiotics, and other substances, then claiming any cellular breakdown proves viral presence. As the rapid evidence review acknowledges, the 1918 Spanish Flu experiments failed to demonstrate person-to-person transmission despite extreme exposure methods, and Christine Massey's 220 Freedom of Information requests found no evidence of proper viral isolation for any claimed pathogenic virus.
What makes HFM particularly interesting from a terrain perspective is its distinct demographic pattern. The disease overwhelmingly affects children under five years old, with peak incidence between one and three years - precisely the age range when children receive the most intensive vaccination schedule of their lives. This timing correlation deserves scrutiny rather than dismissal, especially when we consider that the symptoms attributed to HFM closely mirror documented adverse reactions listed in vaccine package inserts: fever, irritability, mouth sores, skin eruptions, and general malaise.
Section 2: The Body's Intelligent Response
From a terrain medicine perspective, what we call hand-foot-and-mouth disease represents not an attack by an external pathogen, but rather the body's intelligent attempt to eliminate toxins and restore balance. Dr. Marizelle Arce articulates this beautifully when she explains that symptoms are "signposts—clear signals from the body that communicate what is happening internally." The characteristic vesicles on hands, feet, and in the mouth aren't evidence of viral invasion but rather purposeful elimination pathways chosen by the body's innate wisdom.
Consider the specific locations where HFM symptoms manifest. The hands and feet represent our body's extremities - areas with numerous sweat glands and acupuncture points that traditional medicine has long recognized as elimination channels. The mouth, our primary interface with the external world through food and breath, becomes inflamed as the body attempts to discharge toxins through the mucous membranes. These aren't random locations attacked by a virus; they're strategic elimination points the body uses when overwhelmed by toxic burden.
The terrain model suggests that young children's bodies, still developing their detoxification pathways, respond to toxic accumulation with these dramatic but ultimately beneficial symptoms. As Dr. Thomas Cowan explains, these symptoms represent "the best thing your body can do, given the situations and the circumstances that you've provided for it." In his 45 years of medical practice, Cowan has observed that "every symptom has a meaning, and it's the body's way of communicating something." The fever helps mobilize the immune system and create an inhospitable environment for pathogens, the vesicles provide a route for toxin elimination, and the malaise forces rest - all intelligent responses, not pathological failures.
When we examine what virologists claim to observe, the truth becomes even clearer. As Mark Gober meticulously documents, when researchers take fluids from sick patients and add them to their cell cultures containing monkey kidney cells, antibiotics, and fetal bovine serum, the resulting cellular breakdown they call "cytopathic effect" occurs even in control experiments without any patient samples. Cowan puts it bluntly: "All you see is cell cultures breaking down... It's total bullshit." The particles seen in electron microscopy that are labeled as viruses are simply what happens when tissue dies - nothing more than cellular debris being misidentified as pathogens.
Section 3: The Vaccine Connection
The timing of hand-foot-and-mouth disease reveals perhaps its most significant pattern - one that medical authorities steadfastly refuse to examine. The overwhelming majority of cases occur in children between ages one and three, precisely when the childhood vaccination schedule reaches its most intensive phase. By age two, children in developed countries have typically received over twenty vaccine doses, each containing aluminum adjuvants, formaldehyde, polysorbate 80, animal proteins, and in some cases, thimerosal. The symptoms that emerge - fever, irritability, vesicular eruptions, and oral ulcers - mirror almost exactly the adverse reactions listed in vaccine package inserts.
Cowan's observation about childhood illness as communication becomes particularly relevant here. He describes treating young patients who couldn't stop screaming after vaccination: "If you're a one-day-old and you come into the world, excited, your parents gave you life, and then they stab you with a needle and inject poison in you, what are you going to do? You could sit them down and say, 'Look, I don't think you should do this'... But you obviously can't, because you can't even talk. So you scream." When parents don't listen to the screaming, the body escalates its communication - producing rashes, fevers, and the constellation of symptoms we label as HFM.
The medical establishment's refusal to investigate this correlation represents willful blindness. No studies compare HFM incidence in vaccinated versus unvaccinated populations. No research examines whether HFM outbreaks correlate with recent vaccination campaigns in daycares or preschools. Instead, we're given the circular logic that it must be viral because multiple children get sick - ignoring that these children often receive vaccines on similar schedules, creating clusters of toxicity that manifest as apparent "outbreaks." As Gober notes, observing people getting sick together doesn't prove contagion: "If a bunch of rats went into a basement full of rat poison, and you went downstairs to find dead rats, would you conclude that they died because of a contagious virus?"
The Control Group Survey of Unvaccinated Americans provides the empirical evidence that the medical establishment refuses to gather. Joy Garner's groundbreaking 2019/2020 study compared health outcomes between the 99.74% vaccine-exposed American population and the entirely unvaccinated, revealing statistics that should end all debate. Among unvaccinated children under 18, only 5.71% had any chronic condition, compared to 27% of vaccinated children. The autism rate in fully unvaccinated individuals who also avoided the Vitamin K shot and maternal vaccines was 0% - zero cases among 1,024 individuals - compared to national rates of 3.49% in 2020.
Most damning for the HFM narrative, the survey found that even minimal pharmaceutical exposures dramatically increase disease risk. Children exposed only to the Vitamin K shot showed an 11.73% risk of chronic conditions - a 344% increase over the baseline 2.64% rate for those with zero exposures. Those exposed to maternal vaccines alone showed a 21.05% risk, a 697% increase. When children received both the Vitamin K shot and maternal vaccines, their risk jumped to 30% - over 1,000% above baseline. These aren't subtle differences requiring statistical manipulation to detect; they're massive disparities that reveal vaccination as the primary driver of childhood illness.
The statistical significance of these findings exceeds the gold standard used in particle physics to prove theoretical particles exist - the "five sigma" threshold representing a 1 in 3,500,000 chance of random occurrence. The CGS calculated the odds that vaccines are not causing over 90% of chronic conditions in adults at less than 1 in 245 quintillion - a number so astronomical it defies comprehension. Yet while physicists accept five sigma as proof for unobservable particles, the medical establishment ignores evidence exponentially stronger for observable, measurable health outcomes in living children.
This data transforms hand-foot-and-mouth disease from a mysterious viral affliction into exactly what terrain medicine predicts: a detoxification response concentrated in the most vaccine-poisoned demographic. The fact that HFM "outbreaks" occur precisely in the age groups receiving the most intensive vaccination schedule isn't coincidence - it's causation hidden in plain sight.
Common symptoms of Hand-Foot-and-Mouth Disease (HFM)
Low-grade fever
Maculopapular or papulovesicular rash on hands/feet
Painful oral ulcerations (mouth sores)
Vesicles that rupture into shallow ulcers
Sometimes lesions on trunk, cheeks, genital area, or associated nail changes
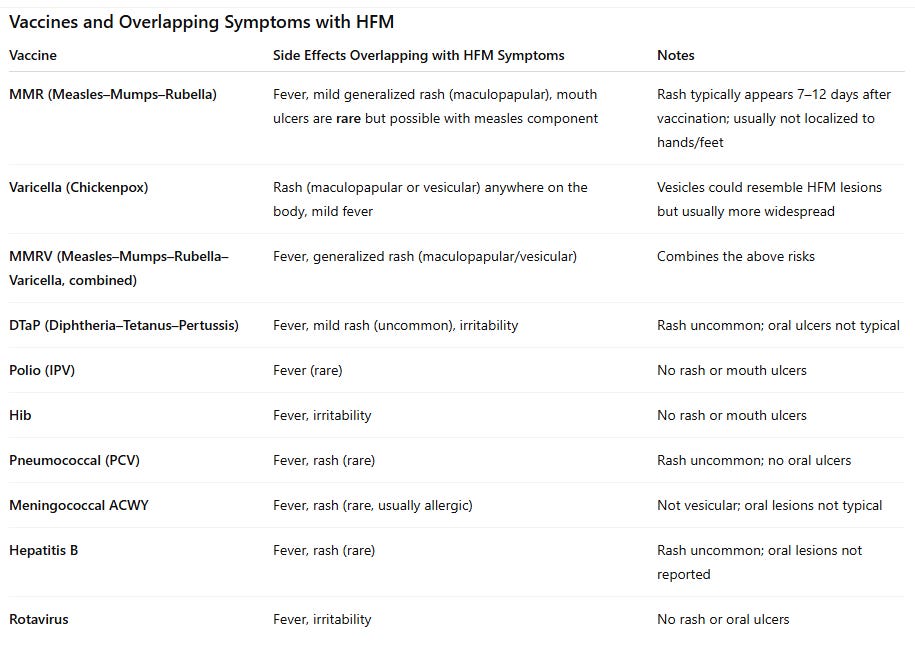
Known side effects of early-childhood vaccines (from official product information, CDC, WHO, and Australian NIP data)
Key Takeaways
Greatest overlap with HFM symptoms: Varicella and MMR/MMRV — these can cause a mild vesicular or maculopapular rash and low-grade fever.
DTaP, PCV, Hib, Meningococcal, Hep B, IPV, Rotavirus — may cause fever, but rash or mouth sores are “uncommon.”
Among the routine childhood vaccines, the ones that explicitly list “mouth ulcers/oral ulceration” in their official fact sheets are the varicella-containing vaccines.
Varicella (chickenpox) vaccine — VARIVAX: the patient leaflet lists a “severe skin rash (ulcers and blistering) … that may involve the … mouth” under rare reactions (Stevens–Johnson syndrome/erythema multiforme). It also lists “mouth ulcer” among reported reactions.
MMRV (measles-mumps-rubella-varicella) — ProQuad: the FDA package insert’s post-marketing section lists “mouth ulcer” under gastrointestinal disorders; SJS and erythema multiforme are also listed in skin reactions. (U.S. Food and Drug Administration)
What’s not listed as causing oral ulcers in their fact sheets: MMR, DTaP, IPV (polio), Hib, pneumococcal (PCV), hepatitis B, meningococcal ACWY, and rotavirus. Their official sheets mention things like fever, general rash, or mouth/throat swelling as part of an allergic reaction, but not mouth ulcers. For example, the current MMR (M-M-R II) US label lists typical reactions but does not list mouth/oral ulcers. (U.S. Food and Drug Administration)
Note: from Official sources
Section 4: The Myth of Contagion
The belief that hand-foot-and-mouth disease spreads from child to child rests entirely on assumption, not evidence. Despite over a century of attempts, no study has successfully demonstrated person-to-person transmission of any disease under properly controlled conditions. The rapid evidence review acknowledges that during the 1918 Spanish Flu, U.S. Navy experiments failed to transmit illness even when healthy volunteers had infected blood injected into them and sick patients coughed directly in their faces. Similarly, Daniel Roytas examined over 200 studies attempting to prove cold transmission and found none that succeeded.
What we actually observe, as Cowan emphasizes, is "two or more people who have the same symptoms at the same time, in the same place. That's what you see. You don't see transmission. You don't see viruses." When children in a daycare develop HFM symptoms, we're witnessing shared exposure to environmental toxins, not viral spread. These environments are saturated with cleaning chemicals, electromagnetic fields from Wi-Fi routers, toxic off-gassing from synthetic materials, and most significantly, children on similar vaccination schedules experiencing similar detoxification crises.
The terrain perspective offers multiple explanations for clustered illness that don't require invoking invisible pathogens. As Alec Zeck outlines, shared exposure to weather changes, seasonal variations in sunlight and vitamin D, collective stress, and even biofield resonance can create patterns that mimic contagion. Gober adds another dimension: "Could the emergence of similar physical symptoms be explained by a hidden interconnectedness between individuals?" The HeartMath Institute has documented heart-rate synchronization among emotionally close individuals, suggesting that what appears as contagion might actually be energetic resonance between human biofields.
Section 5: Addressing the Objections
Critics of the terrain perspective raise predictable objections that deserve honest examination. The most common: "But unvaccinated children get HFM too." This may be true - and it would be entirely consistent with our understanding. Unvaccinated children still face environmental toxins: glyphosate in food, electromagnetic radiation, industrial chemicals in water and air. The difference is that unvaccinated children typically experience milder symptoms that resolve faster - their bodies aren't overwhelmed by the additional burden of vaccine toxins.
The reality that the medical establishment desperately conceals is that unvaccinated children have become vanishingly rare - representing only 0.26% of the American population. The Control Group Survey had to conduct a nationwide search across 48 states just to find enough unvaccinated individuals for statistical analysis. In states like Iowa and Mississippi, the numbers dropped so close to zero that researchers abandoned attempts to locate any unvaccinated persons. This near-extinction of the unvaccinated control group serves the pharmaceutical narrative perfectly - when 99.74% of the population is vaccine-exposed, every disease can be blamed on the tiny fraction who opted out.
The media's fear-mongering about "unvaccinated disease spreaders" relies entirely on anecdote, never data. They'll breathlessly report a single unvaccinated child with HFM while ignoring that the other 99+ children in the daycare outbreak were fully vaccinated. They'll never mention that HFM is almost exclusively - if not entirely - a disease of vaccinated children. The Control Group Survey found that unvaccinated children simply don't manifest these supposedly "highly contagious" conditions at anywhere near the rates of their vaccinated peers. When only 5.71% of unvaccinated children have any chronic condition compared to 27% of vaccinated children, the idea that the unvaccinated are disease vectors becomes laughable.
This statistical sleight of hand - using the 0.26% as scapegoats for diseases overwhelmingly affecting the 99.74% - represents perhaps the most audacious gaslighting in medical history. Every HFM "outbreak" in a daycare, every cluster of sick children in a preschool, is fundamentally a gathering of vaccine-injured children experiencing synchronized detoxification. The unvaccinated child, if one even exists in these settings, becomes the convenient excuse to avoid examining why dozens of "protected" children are simultaneously ill.
"What about historical records of HFM before modern vaccines?" Hand-foot-and-mouth disease as a distinct diagnosis only emerged in 1957 in New Zealand, coinciding with the expansion of childhood vaccination programs following the polio vaccine rollout. Before this, similar symptoms were likely categorized differently or seen as normal childhood detoxification responses to environmental stressors of their era - industrial pollution, DDT exposure, poor sanitation. The medical establishment's need to categorize and name every symptom pattern as a distinct "disease" serves the disease branding agenda, not biological reality.
"If it's not contagious, why do outbreaks follow patterns?" Patterns exist because groups share exposures. When a daycare schedules vaccination catch-ups before school starts, multiple children receive toxic injections within days of each other. They breathe the same air contaminated with cleaning chemicals, play on the same surfaces treated with antimicrobials, eat the same processed snacks, and experience the same electromagnetic bombardment from Wi-Fi routers. As Cowan reminds us, observing patterns doesn't prove causation - it merely shows correlation.
"Doctors and scientists can't all be wrong." This appeals to authority while ignoring history's graveyard of discarded medical "truths." Doctors once prescribed mercury for teething, performed lobotomies for mental illness, and endorsed cigarettes. As Gober documents, the "science of influence" has captured medical education so thoroughly that most doctors never question foundational assumptions. They're not lying - they're true believers in a false paradigm, having never been taught to examine virology's fraudulent methodology.
"But antibody tests show immune response to specific viruses." Antibody tests detect proteins, not viruses. These proteins could be cellular debris from the detoxification process, responses to injected foreign proteins from vaccines, or markers of terrain imbalance. Without ever isolating an actual virus to validate against, antibody tests are meaningless theater. As Christine Massey's 220 FOI requests proved, no health agency anywhere has a properly isolated virus to serve as a gold standard for any test.
"What about the electron microscope images?" Those images show cellular debris, not viruses. Stefan Lanka's control experiments produced identical "viral" particles without any patient samples - just by stressing cells with antibiotics and starvation. The particles virologists photograph are simply what dying cells look like, whether from supposed "infection" or from laboratory poisoning. Calling them viruses is interpretation, not observation.
The most insidious objection comes from parents themselves: "Are you saying I poisoned my child?" This defensive response prevents honest examination of evidence. Yes, well-meaning parents following medical advice have unknowingly allowed their children to be poisoned. Acknowledging this isn't about blame but about breaking the cycle. As Cowan observed with his young patients, once parents understand what's really happening, children often stop needing to "scream" through symptoms to get attention. The healing begins with truth.
Section 6: Disease Branding in Action - The Media's HFM Campaign
The recent surge in hand-foot-and-mouth disease reporting across multiple countries reveals a masterclass in what pharmaceutical marketing calls "disease branding" - selling fear of a condition to create demand for medical interventions. As documented in August 2025 alone, coordinated media stories appeared in India, Canada, Thailand, and the United States, all following an identical script: mysterious outbreaks, worried parents, expert doctors warning of contagion, and calls for increased vigilance. This is no coincidence - it's the "science of influence" that Alan Cassels warned is "40 years ahead of the science of evidence-based medicine."
The formula is predictable. First, create alarm with headlines about "surges" and "outbreaks." The Indian Express breathlessly reports doctors seeing "5-6 cases a day" - hardly an epidemic, yet presented as crisis. Fox News amplifies fear with mentions of a "possible fatal case," burying the fact that serious complications are vanishingly rare. The articles quote concerned doctors like Dr. Manish Mannan explaining how the "virus transmits through direct contact," while Dr. Dhiren Gupta warns of increasing numbers, though never providing context that these mild symptoms have always existed in children.
What these orchestrated media campaigns systematically omit is more revealing than what they include. Not one article mentions that HFM symptoms mirror vaccine adverse reactions. None question why cases predominantly affect recently vaccinated age groups. The Canadian piece casually mentions children returning from summer - when many receive catch-up vaccines for school - yet never makes the connection. The Thai article notes 15,753 cases in children under 4, precisely the most heavily vaccinated demographic, without a hint of correlation. This is disease branding at its finest: control the narrative by controlling what questions are never asked.
The economic machinery behind these campaigns becomes clear when we understand, as revealed in "Selling Sickness," that Merck's CEO dreamed of "making drugs for healthy people, to sell to everyone." Creating fear of HFM serves multiple purposes: it reinforces belief in viral contagion, justifies continued vaccination (never mentioning vaccines as a potential cause), and primes the market for future interventions. As Edward Bernays advised in "Propaganda," you must "sell the vision that will lead to desire for the product, with the consumer believing that it is their own idea." Parents demanding protection from this "highly contagious" disease will never question whether the protection itself - vaccines - might be the cause.
Most insidiously, these articles universally recommend the same ineffective responses: hand washing, surface disinfection, and isolation - none of which address the actual cause if HFM represents vaccine-induced detoxification. By focusing entirely on preventing "spread," they ensure parents never consider stopping the poisoning. The medical establishment has perfected what Christopher Shaw calls "flawlessly executed" disease branding - create the problem through vaccination, rebrand the body's detox response as a contagious disease, use media to amplify fear, then offer more medical interventions as the solution. It's a perpetual profit machine built on parental terror.
Section 5: Understanding True Healing
From a terrain medicine perspective, suppressing hand-foot-and-mouth symptoms with fever reducers, topical steroids, or antibiotics represents a fundamental misunderstanding of the healing process. These interventions stop the body's intelligent detoxification efforts, driving toxins deeper into the tissue where they can cause more serious problems later. As Dr. Arce explains, antibiotics and antimycotics are "highly toxic" substances that force the body to adapt in potentially harmful ways, transforming beneficial microorganisms through pleomorphism into more problematic forms.
Cowan's clinical experience illuminates what happens when we interfere with the body's wisdom: "You can kill [the bacteria] with that chemical, and then that bioremediation will stop, and you'll be left with dead tissue there that won't recycle. Your symptoms will be better because the symptoms come from the recycling, the bioremediation process." He observed that patients who suppressed strep throat symptoms with antibiotics inevitably got recurrent infections, while those who allowed the process to complete naturally never had the problem again. The antibiotics didn't cure anything - they stopped the body's regeneration process, leaving toxic debris that would eventually demand another cleanup attempt.
True healing requires supporting rather than suppressing the body's efforts. This means providing clean water - ideally structured water as described by Gerald Pollack - to help cells maintain their crystalline gel structure essential for proper function. It means removing electromagnetic stressors, particularly in children's sleeping areas where Wi-Fi routers and smart devices create constant disruption to cellular communication. Most importantly, it means addressing the emotional and psychological terrain. As Cowan discovered, children often stop their disruptive symptoms the moment someone acknowledges their distress: "Let me talk to the parents. You don't have to scream to get their attention. I'll tell them that they can't do this anymore."
Section 6: Reclaiming Our Children's Health
The hand-foot-and-mouth disease narrative represents everything wrong with modern medicine - a system that creates illness through toxic interventions, misidentifies the body's healing responses as disease, then profits from suppressing those very responses. As Cowan observes, "There's nothing in conventional medicine that's about healing. It's just stopping the body's regeneration processes." The medical establishment has transformed childhood detoxification crises into profitable "infectious diseases," ensuring parents remain trapped in cycles of fear and dependency.
Breaking free requires what Dr. Arce calls becoming "the Grand Master of your own health" - taking full responsibility for understanding your body's language and supporting its natural processes. This means rejecting the victim consciousness that diagnoses create, recognizing that symptoms have meaning and purpose. When we stop seeing our children as victims of random viral attacks and start understanding their symptoms as intelligent responses to environmental insults, everything changes. The fear dissipates. The agency returns.
The path forward is clear, though it requires courage to walk it. Stop poisoning children with vaccines that contain aluminum, formaldehyde, and foreign DNA. Create environments free from electromagnetic pollution and chemical toxins. Feed them real food, not processed substitutes laden with glyphosate and synthetic additives. Most crucially, listen to what their bodies are trying to communicate. As Gober reminds us, consciousness itself plays a fundamental role in health - our beliefs and fears can literally manifest as physical illness. When we release the fear of contagion and embrace the wisdom of the terrain, we reclaim not just our children's health but their entire future. Hand-foot-and-mouth disease isn't something that attacks our children - it's their bodies' attempt to heal from what we've allowed to be done to them. Once we understand this, we can finally stop the cycle and allow true healing to begin.
Section 7: A Parent's Practical Protocol
When your child manifests hand-foot-and-mouth symptoms, remember: these are signs of the body's intelligence at work, not an enemy to fight. As "The Unvaccinated Child" treatment guide emphasizes, supporting rather than suppressing these processes allows true healing. Based on the book, here's how to help your child through this detoxification crisis while avoiding the trap of symptom suppression.
Immediate Support During Active Symptoms:
Rest is paramount - not as punishment but as medicine. Create a healing sanctuary where the child can direct all resources toward detoxification. As the treatment guide notes, "By lying in bed and resting, we allow those resources to be used for fighting infection and re-establishing normal health." Low-energy activities like audiobooks or gentle music are fine, but limit screens which add electromagnetic stress.
For fever, remember Cowan's wisdom that it represents the body doing exactly what it's designed to do. Support fevers below 104°F with hydration and cool cloths rather than suppressing them with medication. The fever helps create an inhospitable environment for pathogens while mobilizing the immune response. Only intervene if fever exceeds 104°F, the child is under 3 months, or concerning symptoms like seizures appear.
Nutritional Support:
When appetite naturally declines, don't force eating - this allows digestive resources to support detoxification. Bone broths provide nutrients without taxing digestion, as they're "rich in nutrients, easy on digestion and healing to the gut." Eliminate dairy, processed foods, and sugar which feed inflammation. Bieler's broth - a simple vegetable preparation - offers gentle nourishment.
High-dose Vitamin C supports the detoxification process - dose in smaller amounts throughout the day using whole food sources where possible. Vitamin D activates immune components, while zinc protects gut integrity. For children, medicinal mushroom glycerites provide immune support in an easy-to-take form.
Physical Remedies for Comfort:
For the painful mouth sores characteristic of HFM, homeopathic Borax 30C can provide relief without suppressing the elimination process. Apply coconut oil mixed with a drop of lavender essential oil to vesicles on hands and feet - this soothes without driving toxins deeper like steroid creams would.
Constitutional hydrotherapy using alternating hot and cold cloths over chest and abdomen "brings oxygen and immune cells to internal organs" while being deeply relaxing. For younger children, cool washcloths on chest and abdomen provide comfort during fever.
The "magic socks" treatment - wet cold socks covered by dry wool socks worn overnight - "can stimulate the immune system, drain congestion from the head and chest, relax away aches, increase circulation and aid in detoxification."
Detoxification Enhancement:
Epsom salt baths draw toxins through the skin while providing magnesium for cellular function. Add a cup to warm (not hot) bathwater and let the child soak for 15-20 minutes. For lymphatic support, gentle dry brushing toward lymph nodes helps circulation of the lymphatic system which lacks its own pump.
Garlic socks - crushed garlic in cheesecloth applied to feet overnight - provides antimicrobial support without internal consumption. As noted in the guide, this allows children to benefit from garlic's "antimicrobial, anti-inflammatory, immune boosting properties" without digestive upset.
Environmental Optimization:
Remove all wireless devices from the child's sleeping area. Turn off Wi-Fi at night. These simple steps reduce the electromagnetic stress that disrupts cellular communication and structured water. Open windows for fresh air circulation, avoiding synthetic air fresheners or cleaning products that add to the toxic burden.
When to Seek Additional Help:
While supporting the body's natural processes, watch for signs that additional support is needed: dehydration from inability to drink due to mouth pain, fever over 104°F that doesn't respond to cooling measures, or any sudden change in consciousness. Find a naturopathic or integrative physician comfortable with high-dose Vitamin C IVs before you need one - these can provide powerful support for severe detoxification reactions.
The Deeper Work:
As symptoms resolve, address the root causes. If vaccines triggered this detoxification crisis, research vaccine detox protocols from practitioners like Dr. Suzanne Humphries or the CEASE therapy method. Build terrain resilience through nutrient-dense foods, structured water, and reducing environmental toxin exposure. Most importantly, trust your child's body wisdom - it knows how to heal when given proper support rather than suppression.
I appreciate you being here.
If you've found the content interesting, useful and maybe even helpful, please consider supporting it through a small paid subscription. While 99% of everything here is free, your paid subscription is important as it helps in covering some of the operational costs and supports the continuation of this independent research and journalism work. It also helps keep it free for those that cannot afford to pay.
Please make full use of the Free Libraries.
Unbekoming Interview Library: Great interviews across a spectrum of important topics.
Unbekoming Book Summary Library: Concise summaries of important books.
Stories
I'm always in search of good stories, people with valuable expertise and helpful books. Please don't hesitate to get in touch at unbekoming@outlook.com
Baseline Human Health
Watch and share this profound 21-minute video to understand and appreciate what health looks like without vaccination.
Wow! EXCELLENT job here! I loved the part about antibiotics stopping the elimination process. I'd never seen it that way before. Your conclusions make PERFECT sense!
VERY rational, LOGICAL, evidence and data-based work here. THANK YOU!!!
"The specific disease doctrine is the grand refuge of weak, uncultured, unstable minds, such as now rule in the medical profession." Florence Nightengale 1860.